Almost everything injected subcutaneously in this space (GLP-1s, healing peptides, growth-hormone secretagogues) goes into the same few square inches of abdomen, week after week. That habit has a well-documented cost, and it is the most studied complication of subcutaneous self-injection: lipohypertrophy.
The evidence base is built on insulin, because insulin has been injected daily by millions of people for a century and the complication has been measured carefully. We lean on that literature throughout and flag where peptides differ. The mechanical part of the story, repeated needle trauma to one patch of tissue, transfers directly to anything you inject.
What lipohypertrophy is
Lipohypertrophy (LH) is a thickened, rubbery swelling of the subcutaneous fat at a site that gets injected over and over. It is not a bruise or a transient welt; it is remodeled tissue you can often feel as a firm lump and sometimes see as a raised patch. Once established, it tends to be less sensitive to the needle, which is exactly why people keep using it: the lumpy spot hurts less, so it gets picked again, and the lump grows.
Two mechanisms drive it.1 The first is mechanical trauma: every needle entry injures the tissue slightly, and repeated injury to the same patch (accelerated by reused, dulled needles) provokes a local fibrotic and fatty overgrowth response. The second, specific to insulin, is the hormone’s own lipogenic action: insulin is a growth signal for fat tissue, so depositing it in the same spot promotes local fat accumulation. Peptides that are not lipogenic do not have this second pathway, but they share the first, and the trauma pathway alone is sufficient to produce the lesions.
Why it matters: erratic absorption
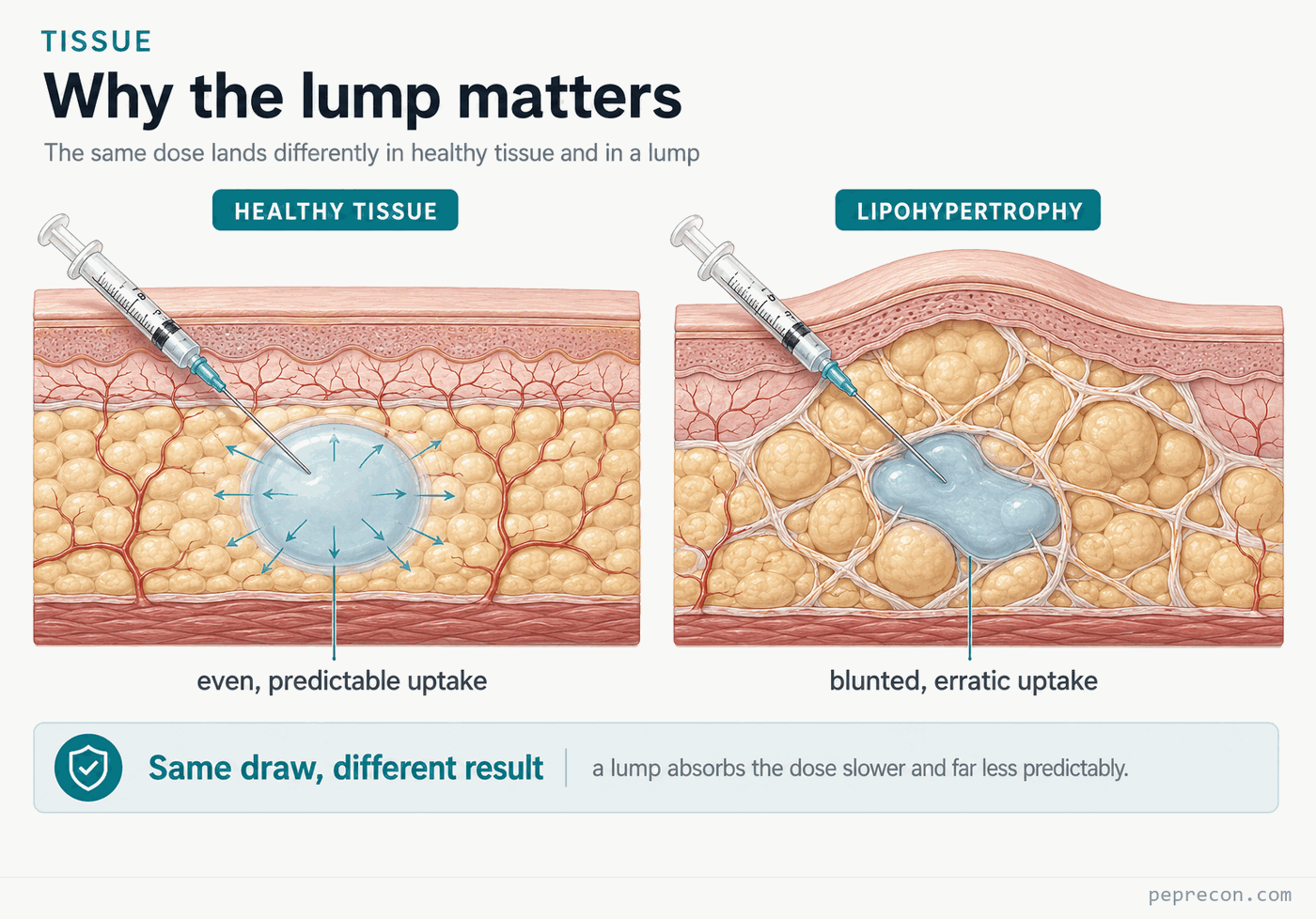
The reason LH is worth caring about is not cosmetic. Lipohypertrophic tissue is poorly vascularized and structurally abnormal, and a drug deposited into it is absorbed slower, less completely, and far less predictably than the same drug in healthy tissue.
The clearest data come from insulin. Injecting into lipohypertrophic tissue produces blunted and more variable absorption and action, and worse post-meal glucose control.2 In a large study of insulin-injecting patients, those with lipohypertrophy had dramatically higher rates of two problems that are downstream of unpredictable absorption:3
For a peptide the consequence is not hypoglycemia, but the underlying failure is the same: you stop knowing how much of a dose is actually reaching circulation. Two identical draws into two different patches of tissue can deliver meaningfully different amounts, which quietly undermines any attempt to run a consistent protocol or interpret your own results. The careful reconstitution math elsewhere on this site assumes the dose you draw is the dose you absorb; lipohypertrophy is the most common way that assumption breaks.
The evidence on rotation
The same body of research that documents the harm also identifies the single most effective preventive: rotating sites correctly.
In the study above, correct rotation was the strongest protective factor against lipohypertrophy. Among patients who rotated sites correctly, only about 5% had LH; conversely, virtually all patients who had developed LH either did not rotate or rotated incorrectly.3 No injectable additive, needle coating, or technique adjustment comes close to that effect size. Rotation is not a nicety; it is the intervention.
How to rotate correctly
“Rotation” has a specific meaning in the injection-technique guidelines, and doing it wrong looks a lot like doing it right. The consensus recommendations below are drawn from the FITTER (Forum for Injection Technique and Therapy: Expert Recommendations) guidance.4
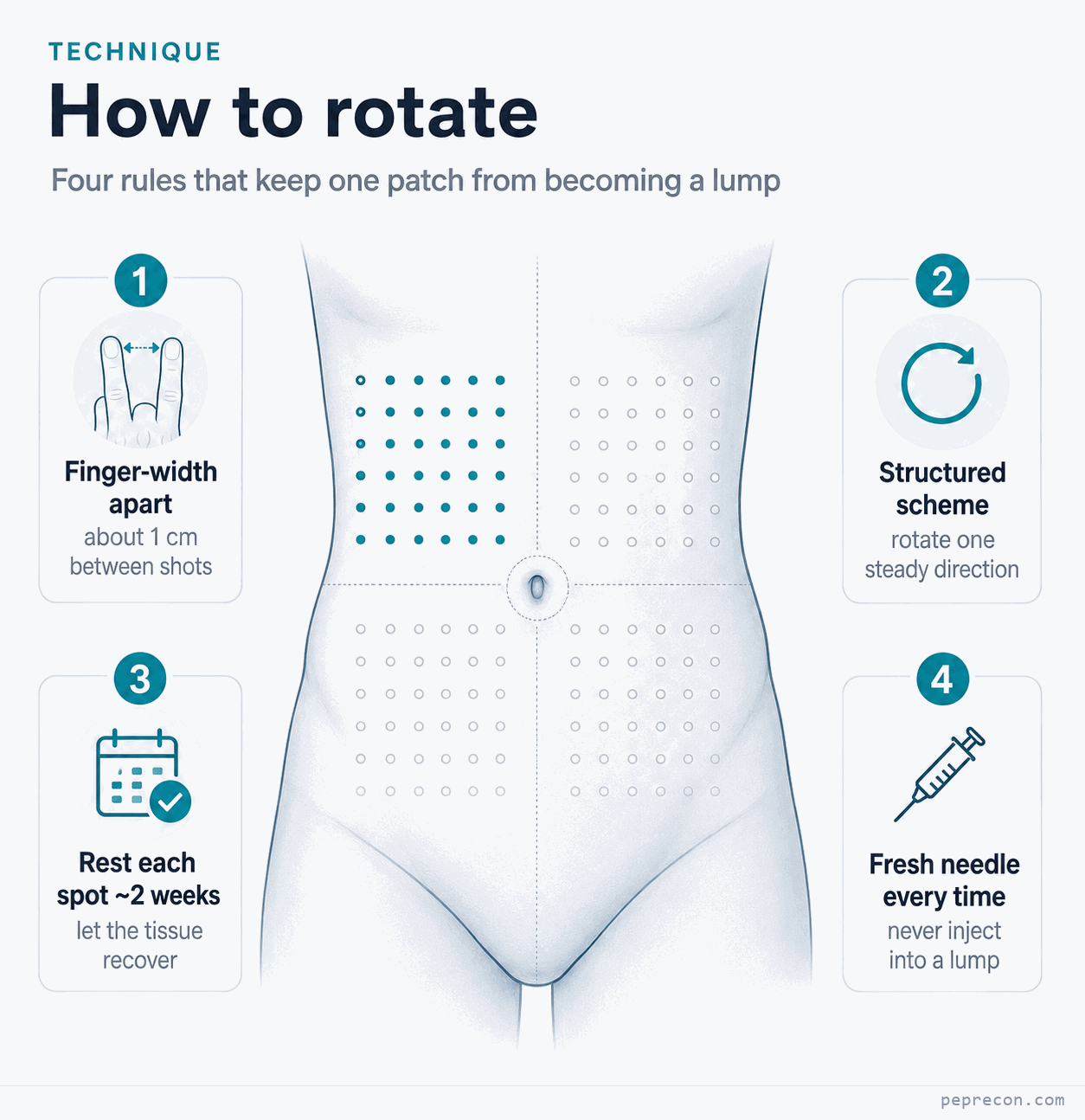
Space each injection at least one finger-width from the last. Roughly 1 cm of separation between punctures is enough to keep from re-traumatizing the same tissue.4 Clustering ten injections inside a coin-sized area is not rotation, even if you move across the room between shots.
Rotate in a structured scheme, not at random. A reliable method is to divide a region into quadrants (or halves, for smaller regions like the thigh), use one quadrant for a week, and move to the next in a consistent direction (clockwise, say) so that you do not return to any single quadrant for several weeks. A structured scheme is what guarantees real spacing over time; “wherever feels fresh” tends to collapse back onto a few favorite spots.
Give each spot weeks to recover, not days. Tissue needs time to heal between punctures. This is the principle behind the cooldown window in our rotation map: the goal is to cycle through enough distinct sites that any one spot rests on the order of two weeks before it is used again. If your injection frequency and the number of sites you use mean you come back to the same patch every few days, the rotation is too tight.
Use a new needle every time. A fresh needle has a sharp, silicone-coated tip; even one use bends the tip and strips the coating, increasing the tissue trauma on the next entry.4 Reused needles measurably accelerate lipohypertrophy, and they hurt more, which again pushes people toward the numb lumpy spots that already have it.
Inject into healthy tissue, and never into a lump. If you can feel a firm or rubbery area, do not inject into it; absorption from it is unreliable. Different regions also absorb at different rates (for insulin, abdomen is fastest, followed by the upper arm, then thigh and buttock), so keeping a given type of injection to a consistent region while rotating within it avoids stacking site-to-site speed differences on top of everything else.4
Recovery
Lipohypertrophy is partly reversible, but slowly. The standard guidance is to stop injecting into the affected area entirely and give it months, during which the tissue gradually remodels back toward normal.4 One practical warning comes out of the insulin world and applies to any potent injectable: when you move off lipohypertrophic tissue onto healthy tissue, absorption improves, sometimes abruptly, because the healthy tissue takes the drug up more efficiently. The same number of units that felt stable in a lump can land differently in fresh tissue, so a switch is a moment for extra attention, not less.
Limitations
A few worth naming explicitly:
- The quantitative evidence is from insulin, not peptides. The prevalence figures, the absorption studies, and the glycemic-outcome numbers all come from diabetes research. The mechanical-trauma mechanism and the rotation principle transfer to any repeated subcutaneous injection; the insulin-specific lipogenic mechanism and the exact magnitudes do not necessarily.
- Peptide injections differ in ways that may help or hurt. Volumes are often smaller and frequencies sometimes lower than daily insulin, which would reduce trauma; but needles are often reused and sites rarely tracked, which increases it. The net effect in this population has not been measured.
- “Recovery time” is not precisely defined in the literature. Tissue healing varies between people; the two-week-per-site target is a reasonable, conservative heuristic, not a measured constant.
Conclusion
Lipohypertrophy is the predictable result of injecting the same patch of tissue repeatedly, and its main harm is not the lump but the erratic absorption that follows: the quiet loss of any guarantee that the dose you drew is the dose you got. The injection-technique literature points to one dominant fix: rotate sites on a structured scheme, space punctures by at least a finger-width, give each spot weeks to recover, use a fresh needle each time, and never inject into a lump. Our rotation map exists to make the structured part automatic.
References
-
The pathophysiology of lipohypertrophy is generally attributed to a combination of repeated local mechanical trauma and, for insulin specifically, the lipogenic (fat-growth-promoting) action of insulin on subcutaneous adipose tissue. See discussions in Kalra S, et al., “Insulin-Related Lipohypertrophy: Lipogenic Action or Tissue Trauma?” Indian J Endocrinol Metab. 2016. ↩
-
Famulla S, Hövelmann U, Fischer A, et al. “Insulin Injection Into Lipohypertrophic Tissue: Blunted and More Variable Insulin Absorption and Action and Impaired Postprandial Glucose Control.” Diabetes Care. 2016;39(9):1486–1492. ↩
-
Blanco M, Hernández MT, Strauss KW, Amaya M. “Prevalence and risk factors of lipohypertrophy in insulin-injecting patients with diabetes.” Diabetes Metab. 2013;39(5):445–453. Reported lipohypertrophy prevalence of 64.4%; correct rotation strongly protective (≈5% LH among correct rotators, while ≈98% of patients with LH did not rotate or rotated incorrectly); unexplained hypoglycemia in 39.1% of patients with LH vs 5.9% without; glycemic variability in 49.1% vs 6.5%. ↩↩
-
Frid AH, Kreugel G, Grassi G, et al. “New Insulin Delivery Recommendations.” Mayo Clin Proc. 2016;91(9):1231–1255 (the FITTER consensus recommendations). Source for finger-width (~1 cm) spacing, structured rotation schemes, single-use of needles, regional absorption differences, and management of established lipohypertrophy. ↩↩↩↩↩